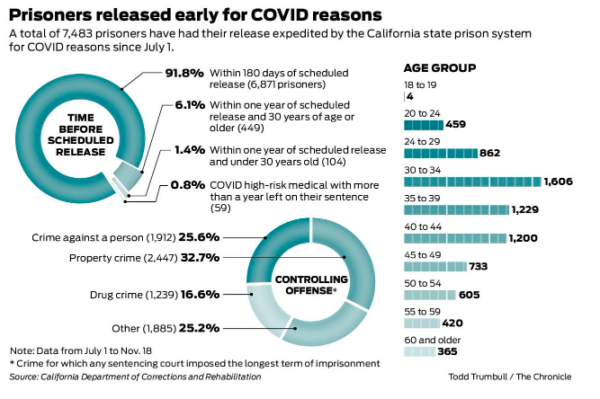
You may recall that the Court of Appeal’s population reduction order in Von Staich did not specify the method by which CDCR should go about population reduction (though it did strongly recommend focusing on people aged 60 and over with 25 years of incarceration behind them.) The order specified that CDCR could choose to comply via releases or transfers. As far as releases, the recent Chron exposé shows that they delivered more or less on what was promised back in July: far too few people, 99% of whom were getting out in a few months anyway, and only 0.8% of whom were COVID-19 risks.
What this indicates–and what the AG’s petition for review to the California Supreme Court indicates–is that CDCR intends to address this crisis almost exclusively via transfers. This is also becoming clearer and clearer in the Marin Superior Court, where Judge Howard, who is presiding over hundreds of habeas corpus petitions from San Quentin, issued the following order:
The gist of the decision is this: Judge Howard is proceeding with fashioning the remedies, as he considers Von Staich “persuasive authority” and despite declarations from the AG that they do not intend to comply until they hear back from the Supreme Court. At the same time, he seems unsympathetic to the arguments against transfers, because the Von Staich decision “provided clear guidance that transfer was a viable remedy.” The AG representatives did state that, independently of the Von Staich decision, they are starting their own transfer initiative, which targets people aged 65 and older. Judge Howard has ordered them to provide a list of the people they are transferring, and the petitioners’ lawyers to compile a list of people who are aged 60 and over and/or have COVID-19 risk factors.
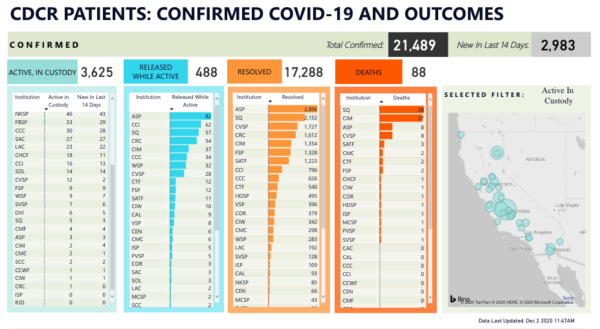
How is this playing out on the ground? You can get a sense from the image at the top of this post. In the last week, per the San Francisco Bay View, people inside–both at San Quentin and at other institutions–have been pressured to accept a transfer out of their own volition, and when they refuse–they are asked to sign the form above, in which they waive any future claims about the risk they face. The form requires them to initial the following statements:
I understand that due to my age, I am at high risk for developing serious complications if I get infected with COVID-19.
I understand that I have one or more medical conditions that makes me high risk for developing serious complications if I get infected with COVID-19.
I understand that COVID-19 could lead to serious complications such as lengthy hospitalizations or even death.
I understand that living in places where individuals are in close contact and physical distancing is difficult to follow, such as prison dormitory [sic], will increases [sic] my risk of being infected by COVID-19.
I understand that COVID-19 could lead to serious implications such as lengthy hospitalization or even death.
I understand that if I change my mind and decided [sic] to be housed in celled housing, I will submit a 7362 or talk to a health staff to request for [sic] celled housing.
I’m hearing from family members and friends of incarcerated people that CDCR is gearing up toward involuntary transfers at Quentin and elsewhere, which are (and always have been) their prerogative, and so, these so-called informed consent forms are actually obsolete. Therefore, it is now more obvious to me than ever that CDCR is worried about a monetary damages lawsuit, and with good reason–I expect we’ll see one in the not-too-far future. If so, I doubt that these waivers, given the circumstances in which they are being procured, will even come close to providing the kind of defense that CDCR, or the AG, think it will provide.
More importantly, the virus doesn’t attend the status hearings at the different courts, and follows its own agenda, which is–as it always has been–to invade cells and replicate itself, which makes this transfer agenda even more inappropriate. As of three days ago, every single CDCR facility has a COVID-19 outbreak, which raises the question–how do CDCR officials purport to improve the situation via transfers, and where are they going to shuffle people to? The information I got from Solano, and a conversation with a relative of someone at SATF, have convinced me that the same pathologies that led to the spread of the virus in San Quentin are now in evidence in other prisons.
Which brings me again to the point of carceral permeability. The logic of lawsuits and court rules doesn’t conform to the realities of geography. By their very nature, they deal with “cases and controversies”, not with proactive solutions to rapidly evolving situations. Order a remedy in one prison, and by the time it’s fashioned, the outbreak will quell there and spike in other places. Exhibit judicial caution and give prison officials the choice between transfers and releases (which is, after all, what courts are supposed to do–express restraint) and they will make the wrong choices. Thinking about this remedy regarding San Quentin alone is part of the brief, but in terms of the actual problem, it makes no sense to implement the remedy in isolation from what is happening in other prisons.
One of the often overlooked aspects of mass incarceration is that, as Erika Camplin puts it, “we as a nation are effectively feeding around 2 million mouths at least three times over each and every day.” Prison food has always been a problem; we even had a conference about it nine years ago. What I remember from the conference is that the CDCR nutritionist spoke on one of the panels and showed slides of prison meals that looked decent enough; under pressure from audience questions, however, she admitted that the slides were doctored, and then lashed out, “these people are monsters.” The rest of the panelists, most of whom were prison and jail doctors, immediately said, incensed, “that’s a lie.”
The pandemic has let things drop far beneath even that already low baseline. During the big outbreak in San Quentin, kitchen workers became infected and fell ill, which led, for several weeks, to serving the men an extra lunch in lieu of a hot dinner (to make up the missing calories.) We now learn from reports of people inside that the same, and worse, is happening at other institutions.
The email chain in the image above is making the rounds on Twitter; I don’t know who sent it around, but here is the text, reproduced. The printout is stamped as “Pelican Bay State Prison, Security Housing C-8.” The first email in the chain is from a Bryan Price to a Chad Parry, CC’ing a David Barneburg. I looked Barneburg up, and it looks like he’s Associate Warden at Pelican Bay. Price writes:
Hey Chad how’s your night going.
Well as for here, it’s not going to good. The inmate are starting to act out over the food and I don’t blame them. I thought when we cut one of their hot meals like dinner. In the past we have given them two lunches for dinner to make up for the calorie lost. Right now they got six crackers, two cookies, a small bag of pretzels, block of cheese and a drink mix. They also got 1 peanut butter, banana and a jalapeno. It is hard to believe that two of these lunches and the breakfast meal has the calories that is due to them. I the memo it states they will be getting box lunches with fruit, milk and juice.
So my question is, is this right because it does not seem right. The same lunch they saw this morning is the one they got for dinner. Hope there is something we can do. I think it’s going to get really bad really fast around here.
Any help in this matter would be greatly appreciated.
Out of the obvious awfulness of the whole thing, for some reason I find myself stuck on the mystery of the jalapeño. What is someone who can’t cook, and who has no access to vegetables, supposed to do with a single jalapeño? Is it cooked? Canned? Pickled? Frankly, I’m not sure the problem is only or even primarily the calories (snacks, peanut butter, and the “drink mix” probably pack a punch of calories)–the serious problem is the nutritional content, which seems sorely lacking.
Chad’s response:
Hey Bryan, that’s the correct meal. They were supposed to get the extra stuff you mentioned… not sure what is planned for tomorrow.
Kim, anything we can do to improve upon this meal? The fellas aren’t enjoying it much…
Thank you
Several family members and friends chimed in the relevant twitter thread. One person reported that she received a letter from someone at VSP who reported that “they are receiving 8 tablespoons of food per meal.”
I’m unsure whether this is garden variety incompetence or pandemic-related; the dinner shortage mentioned in the first email suggests the latter. This is pure conjecture, but the numbers of infected staff have shot up, which could explain kitchen worker shortage. I’m also unsure who leaked this printout; it features pretty feeble efforts to mask people’s names, but not their emails, so the names were easily readable.
Today feels like we’ve crossed a new threshold of horror: As of this morning’s update of the official CDCR ticker, every single CDCR facility has a COVID-19 outbreak. Every single facility has new cases from the last 14 days. There are currently 4,763 active cases in custody. So far, 24,716 people–more than a quarter of the current prison population–have contracted COVID-19 behind bars, and 93 people have died in 17 facilities.
Numerous prisons are seeing major outbreaks (more than 50 new cases in past 14 days): CCI (92 new cases), LAC (198 new cases), SAC (103 new cases), CAC (174 new cases), CEN (319 mew cases), CTF (393 new cases), HDSP (464 new cases), KVSP (92 new cases), MCSP ( 469 new cases), NKSP (77 new cases), PBSP (51 new cases), PVSP (699 new cases), SATF (937 new cases), and VSP (339 new cases). There are new outbreaks at CIW (37 new cases–a third recurrence!), CMC (38 new cases), SOL (34 new cases), CCWF (3 new cases), DVI (11 new cases), ISP (12 new cases), RJD (3 new cases–the last prison to see an outbreak), SVSP (27 new cases), SCC (16 new cases), and WSP (22 new cases–a recurrence.)
All facilities have staff cases. So far, 7366 prison staff members have contracted COVID-19 behind bars; 1722 of these are new cases and 2121 are still deemed “active cases.” Ten staff members have died.
Big facilities have cases. Small facilities have cases. Overcrowded facilities (20 prisons are still over 100% capacity!) have cases. Facilities under, but close to, 100% capacity have cases.
I look at this and think of the Attorney General’s stance in the Plata, Von Staich, and Hall et al. cases. “We can safely transfer people; your suggestion that we cannot is not well taken.” Transfer them where?
Nor is testing a silver bullet; it merely helps the analysis after the fact. Mule Creek, which features 469 new cases, has tested 95% of its population. Testing itself, without decisive action, is a diagnostic, not a prevention mechanism.
An acquaintance at Solano prison managed to send me a missive through a common friend. I’ve removed his identifying information, and this is what is happening there:
Current conditions at CSP-SOL
Complaints: 1. Buses have arriving with inmates from prisons where known positive coronavirus cases have been documented.
2. CDCR are not quarantining these inmates as they arrive, exposing the entire housing units to potentially dangerous viruses.
3. CSP-SOL is currently experiencing an outbreak
4. C/O’s are working double shifts some of them, going from an infected building to a non-infected bldg exposing inmate population to higher levels of probable infection.
5. C/O admitted that a staff member was covid positive a d thus potentially started the spread/outbreak.
6. Inmates have been forced to move from one to another to facilitate work assignments or receive a CDCR RVR115, for refusal or asking for a job change.
These issues and there are more, are some of the things the guys want the public to know.
We are given the proper PPE’s (only received them 2 days ago, before that we only had inmate-made masks), it’s just a mess.
And in the face of this, California Attorney General Xavier Becerra, who has been presiding over the state’s outrageous, self-righteous responses to this plight, is rewarded with a cabinet seat–the health seat, in the name of all that is holy?
Something is rotten in the state of California. Rotten throughout, from top to bottom. In today’s post I juxtapose for you four pieces from the last couple of days, which illuminate just how much trouble we’re in.
Scene 1: The SATF Horror and the Geography of Prison Remoteness
Throughout the summer, the public gaze was laser focused on San Quentin. There was a good reason for this; at 2,239 cases and 29 deaths, the outbreak at Quentin was the worst COVID-19 outbreak in the nation and the worst medical prison disaster in the country’s history. But as has been the case throughout this ordeal, once attention turns somewhere, the government’s or anyone else’s, the virus has already found opportunities elsewhere. By the time the litigation surrounding the Quentin catastrophe matured into an order and started moving toward fashioning remedies, the pestilence metastasized elsewhere–whether through a careless employee or a botched transfer, we won’t know. The CDCR population infection count shows numerous large outbreaks, to the tunes of hundreds of people, in prisons located in rural areas. Jason Fagone’s recent Chron story turns the focus to the Substance Abuse Treatment Facility (SATF) in Kings County, the largest prison in the state, which is operating at 128% of capacity. Not only is the outbreak there horrible, and has already claimed lives, but the conduct of prison authorities there seems absolutely appalling:
In just the past two weeks, 713 men in custody at SATF [now 851 – H.A.] have tested positive for the coronavirus, according to CDCR’s web tracker, and as of last week, 150 staff members were infected. Half of the facility’s 4,400 prisoners have caught the virus since August. Three have died.
One day last week, when prison staff tried to move a new man into an empty spot in Meyer’s eight-man cell, he got nervous, he said in an interview via JPay, a prison email service. Days earlier, another man sleeping mere feet away from Meyer had developed COVID-19 symptoms and was removed by staff, and Meyer suspected that his new cellmate might also be infectious. Meyer approached the officers’ station and complained, saying he didn’t want to be housed with a potentially contagious person. That’s when he was handcuffed, Meyer said.
Two days ago I talked with Sam Lewis of the Anti-Recidivism Coalition about the possibility of a vaccine for incarcerated populations, and one of the points he brought up was the proximity of San Quentin to white, wealthy Marin County. I think Sam was right to say that Quentin receives an inordinate amount of attention, but I suspect race and class play into this situation in ways that have more to do with political culture, proximity, and opportunity. Quentin is extremely close to the Bay Area, where all kinds of do-gooders like me have easy daily access to the prison; if there’s no traffic, it takes approximately 35 minutes to drive to Quentin from my house. Given that, for decades, prison programming has been slashed–most recently, this was one of the negative effects of the recession–the availability of a cadre of academics and activists as volunteers produces aricharrayofprogramming (go ahead, click on each link, and I could offer more.) Because parole hearings emphasize programming and encourage people to talk in “programspeak”, and because of the paucity of programming elsewhere in the system, people are desperate to come to Quentin and avail themselves of these opportunities as much as they can if they ever want to be approved for parole.
By contrast, California’s other large prisons are located in rural areas, mostly in poor towns that were persuaded to accept prison siting and become a “company town” because of the promise of jobs. These places are not squeaky wheels, and for Bay Area or Los Angeles do-gooders they are difficult to access. For example, during the Pelican Bay hunger strike, my students had to drive 8-9 hours to visit the strikers, which implies huge barriers for visitors without the means to drive or stay at a hotel. These places are not “squeaky wheels”, and it’s quite difficult to get the programming “grease” there. Also, it means that the voices raising serious concerns about the outrages that happen in these rural prisons are far less amplified by voices of high-profile, concerned progressive politicians.
Scene 2: Inaction Figures
The Chronicle is on a roll, continuing with a hard-hitting, data-intensive piece by Nora Mishanec. Mishanec managed to obtain a demographic breakdown of the thousands of people who were released by CDCR since Newsom promised 8,000 releases by the end of the summer. It’s not summer anymore, of course, and even when the plan was proposed it was already underwhelming–too little, too late, too piecemeal, and too restrictive. I am sorry to say that this sad excuse for pandemic relief played out exactly as I had predicted, and please believe me that I take no pleasure in having been 100% right.
This graphic from the Chron story gives you an idea of who was released and who was not. Take a look at the circle in the top left. The vast majority of people who have been released had only months left on their sentence back in early July. It is now early December, and these folks would have gotten out by now anyway–they just got a wee push on the way out the door to hasten their release. This is something that happens all the time in California prisons, pandemic or no pandemic: every month thousands of people churn in and out of the system, the folks whose sentences have ended to be exchanged for folks coming in from jails (The population reduction here is artificial, and stems from the halt of transfers from jails–but the carceral apparatus as a whole is bursting at the seams, and of course now the jails are seeing their own COVID-19 horrors and are grossly over-capacity. Something’s gotta give, and there are already jail lawsuits.) Only 0.8% of the people who were released were deemed “COVID high-risk medical”, when a full quarter of the population on the eve of the pandemic was people aged 50 and over.
Why, you might wonder, are so few of the people who got released in the over-50 bracket (1,390 out of 7483)? The answer is in the bottom right. People convicted of violent crime who, unsurprisingly, serve longer sentences and, also unsurprisingly, are older because of it, are underrepresented. Those are also the folks at highest risk of contagion and serious complications. But this plan was not designed with public health in mind–it was designed to avoid headlines like “Newsom Releases Murderers, Yikes.” And so here we are.
Scene 3: Insult to Injury
If they’re not laboriously and efficiently going over people’s files and releasing grandparents back to their families, what, pray tell, are state officials busy doing? I’m so glad you asked: The best and brightest at the California Attorney General’s Office are busy not only petitioning the California Supreme Court to review the population reduction order in Von Staich and jamming the wheels on hundreds of habeas petitions, they are petitioning the court to depublish the decision itself. Yes, you heard it right. Dozens dead, tens of thousands infected, and the most pressing order of business is to obliterate from bureaucratic memory that there were compassionate, humane, knowledgeable judges, who recognized a human rights crime when they saw one, and acted accordingly.
You are incredulous? I get it. So was I. Here’s the whole thing for you to read.
What more is there to say about this? At every junction, when the opportunity emerges to do the right thing, these folks are doing the exact opposite. We are going to pay dearly for this concerted cruelty when the time comes to get buy-in for vaccination (that is, if anyone there might ever see prisons for what they are, which is confined, crowded spaces, and actually prioritize “murderers, yikes.” Want to know why it is important to vaccinate? here’s my op-ed in the Chron about this.) By the time the vaccine comes to the prison gate, people will not believe CDCR that it is in their benefit to take it, and while I find this awful and deeply disappointing, I deeply understand where the suspicion and resentment come from.
Scene 4: No Bad Deed Goes Unrewarded
What is going to happen to all these folks, who have worked so hard for months to keep aging, infirm people languishing behind bars, vulnerable to the pandemic? Gosh, I’m so glad you asked, because California’s AG Xavier Becerra, whose signature decorates everything you’ve seen defending CDCR in courts since March, is being tapped for a position in the Biden cabinet.
Look, I’m not a member of the no-lesser-evil brigade, and in November I cheerfully and without reservations voted for Democrats, even Democrats who have deeply disappointed me, because the alternative was to keep a despotic, sociopathic, semiliterate career criminal in office. For four years I was a vortex of disdain for the repertoire of cruelties of the Trump Administration, and I’m thrilled the people I voted for won. Elections are a buffet at a roadside motel, not a personalized meal. But when you’re handling what we call a “Big Bad” in TV tropes, the other side automatically becomes “the good guys,” and critique of them is muted, or at least softened–even when the courageous leaders of La Résistance forget about the burden of proof or flip-flop about the death penalty. I suspect it won’t be long before we forget how Monsieur et Madame Blanchisserie Française, the delectable taste of Yountville gastronomy still fresh in their mouths, proceeded to close our children’s playgrounds with not a shred of medical evidence connecting them to outbreaks. I get it. We’re grownups, politicians are politicians even when they are generally on the right side, and people should not be expected to be perfect. But I’m frustrated that the nature of California politics creates the illusion that we are a blue, progressive state, in the face of everything that has been going on.
Why is it that we appear so blue when our prisons are such a horror show? My colleague Vanessa Barker offers a convincing explanation. By contrast to the East Coast, or even the Pacific Northwest, California’s political culture is both deeply polarized and populistic. Our red counties, which are, after all, where most of our prisons are, are deeply red; jails there are run by red sheriffs and prisons by red CDCR officers. A lot of decisionmaking happens on a local level. Even when a prison is located in a blue county, such as San Quentin in Marin, prison officials refuse to collaborate with county health officials, citing jurisdiction. Moreover, we tend to legislate our criminal justice arena via referendum, which creates a lot of the horrors that I recount in Chapter 2 of Yesterday’s Monsters: a salience of a particular class of victims as the moral interlocutors of criminal justice, inflammatory rhetoric, and a lot of money backing up fear and hate.
The consequence of this is that our elected officials, who are so right on so many things (immigration, healthcare, climate action) are so often so wrong about criminal justice. Some of what we have going on is so deeply ridiculous–to name just one example, moratorium on a death penalty that should have been abolished eons ago, and because of populist stubbornness we can’t reap the huge economic benefits of abolition–and it is difficult to explain to lefty friends on the opposite coast how come people who appear to be such heroes on the national stage act in such villainous ways on the local stage.
This week, I recommend that you keep your gaze on some of the newest outbreak sites. Beyond SATF, there are also serious outbreaks in PVSP (643 new cases), HVDP (473), MCSP (416), CTF (284), and VSP (298). Dozens of other facilities have “only” dozens of cases. The only CDCR facility with no cases at present is RJD. The death toll systemwide has risen to 90.
Tomorrow at noon I’ll be talking with Sam Lewis from the Anti Recidivism Coalition (ARC) about the imperative to prioritize incarcerated populations as recipients of the COVID-19 vaccine – for the sake of all of us.
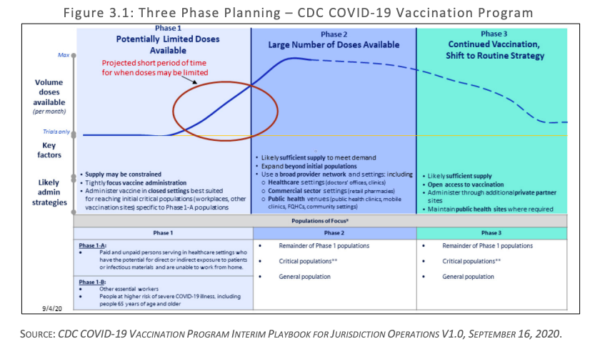
I’m getting a lot of phone calls from journalists about the California Department of Public Health’s COVID-19 vaccination plan, which you can find here in its entirety. The state vaccination plan consists of three phases (see the image below).
Phase 1, during which the state will have a limited supply of vaccines, focuses on critical populations in two subphases:
Healthcare personnel likely treating patients with COVID-19 (Phase 1-A)
Healthcare personnel likely to be exposed to COVID-19 (Phase 1-A_
People at increased risk for severe illness or death from COVID-19 (Phase 1-B)
Other essential workers (Phase 1-B)
California has an Allocation Data Team tasked with identifying these critical populations. CDCR is mentioned as one of the agencies whose datasets are going to be reviewed by the Allocation Data Team. Notably, one of the criteria for allocating vaccines is “identifying disadvantaged populations and communities that have been disproportionately impacted by COVID-19 in terms of higher rates of infection, hospitalization, and deaths.” To combat these well-documented disparities, California has developed a health equity metric and is working to improve the collection of race and ethnicity data associated with testing and cases.
Part and parcel of the vaccination plan is an effective communication strategy, which consists of outreach and education. The report explains how communication will be carried out:
With over 4,000 medical providers participating in California’s Vaccines for Children program and over 500 federally qualified health centers in our Vaccines for Adults program, a solid communication infrastructure exists for getting information and program updates to participating providers (program updates are sent electronically and also posted at https://eziz.org/ ). The CDPH Immunization Branch also employs field staff in five regions to serve as liaisons between provider offices and local health departments. These mechanisms, combined with the knowledge and relationships between local health care providers, pharmacies, and local health departments, have already established points of contacts and methods of communication. Additionally, local emergency preparedness programs have established close communication channels with first responder organizations, groups serving vulnerable populations and large employers throughout our state’s diverse counties. Local health departments have also been keeping close track on communities most adversely affected by COVID-19 and many have bolstered their responses to include specific outreach, education and mitigation efforts in those communities, establishing good relationships along that way that are paving the way for COVID-19 vaccine.
We have also been working with the California Conference of Local Health Officers and the County Health Executives Association of California to define and establish contacts for Multi County Entities (MCEs). An MCE is a health system that has facilities in more than two California counties to centrally support local implementation in all of its locations, set policy for all of its facilities, order and store vaccine, has a centralized pharmacy, and has a demonstrated track record in immunizing all of their staff. Northern and Southern California Kaiser Health Systems are the two largest MCEs defined to date. Conversations are continuing to delineate more MCEs and processes are being created and refined for how these entities will be registered in our provider enrollment systems for vaccine ordering, allocation, tracking and reporting. MCEs will become critical partners to immunizing in their communities and will be brought fully into all communication networks and monitoring infrastructures. We will augment these well-established networks with any additional input from our Community Vaccine Advisory Committee.
Successful communication regarding critical population groups will start with clear guidance at the state level. The state will communicate to local health jurisdictions and MCEs about which and when specific critical populations should be receiving the vaccine. The state, in turn, will rely heavily on these local jurisdictions and multi-county entities to communicate directly with the providers for whom they will be approving allocations. The points of contact for these providers will be established through the provider registration process, which is discussed in further detail in Section 5.
Additionally, we will employ various communication methods to reach critical population groups. To communicate out to the groups that will be eligible for vaccination, we will send messages both from the local and state level about which categories of people should be vaccinated and, when. At the local level, emergency operations centers remain activated and will utilize well-established networks for reaching emergency responders and health care personnel. These well-established networks include Public Health and Medical emergency response partners, such as the Regional Disaster Medical Health Coordination and Medical and Health Operational Area Coordination programs. We will rely heavily on these networks as well as on statewide health care associations such as the California Hospital Association, the California Primary Care Association, the California Medical Association, local health care coalitions, and others. We will also rely on the California Immunization Coalition, our CCLHO and CHEAC organizations, EMS organizations (such as the Emergency Medical Services Administrators’ Association of California [EMSAAC] and the EMS Medical Directors Association of California [EMDA]), and many other professional associations. Emphasizing transparency and equity every step of the way, we will engage our Office of Health Equity, Governor’s COVID-19 Vaccine Task Force, Community Vaccine Advisory Committee members and other stakeholders to ensure that our communications are inclusive and that our strategies are in alignment with the best use of the vaccine at any given point in time.
This report, to me, raises a few points that are crucial to highlight at this particular time–and that require immediate action:
Prisons MUST be designated a vaccine priority site because of the nature of the interpersonal interactions.
Everything we know about the pandemic in prisons shows us that the rate of infections is much higher–approximately ten times higher–than the rate in California generally, and that mortality rates–even when adjusted for age–are much higher. Prison staff–correctional officers and prison workers–come in direct contact, and treat, incarcerated COVID patients just like healthcare personnel on the outside. Moreover, incarcerated people have not seen their families and loved ones since early March, when all visitation was halted because of the pandemic. Vaccinating them should be a priority.
Prisons MUST be prioritized because vaccinating behind bars protects everyone in CA.
Moreover, it is imperative to understand the role that prison outbreaks play in the overall COVID picture of the state. As of today, only two CDCR facilities do not have any cases, and numerous prisons have serious outbreaks with hundreds of cases. The analysis we have provided throughout the last months shows a correlation between spikes in CDCR COVID rates and spikes in the surrounding and neighboring counties. Prioritizing prisons as vaccination sites protects everyone in California.
If equity is a consideration, incarcerated people should be first in line to get vaccinated.
The California Department of Health plan rightly emphasizes the need to factor equity in the distribution of vaccines, specifically through the prioritization of communities and race/class demographic groups who have born the brunt of infections and deaths so far. I can hardly think of a category of Californians who have, disproportionately, suffered more from COVID than incarcerated people. Vaccinating them first is not only prudent and worthwhile–it is fair.
At the same time, from a public health standpoint, outreach and education must begin now.
There are three main populations behind bars: incarcerated people, prison workers, and correctional officers. For reasons that I explained here, there is a serious, and understandable, trust and legitimacy deficit that could hinder effective cooperation in getting the prison population vaccinated, which stems from the fact that, for months now, whenever CDCR had an opportunity to earn trust and engender good will, they did exactly the opposite. CDCR have to start working on repairing this fundamental trust breakdown right now. The best way to do it is to drop all appeals, petitions, grandstanding, performative protestations about public safety, and resistance to the idea of releases, and let aging, infirm people go immediately home to their communities. Not only will this help get the pandemic under control much more quickly, it will go a long way toward reversing the understandable sense among the prison population that CDCR is deliberately indifferent to their plight, and thus will contribute to raising vaccination rates.
The other problem I foresee is with collaboration and buy-in from correctional officers. As I explained here, instead of raising the alarm about the health risks to their membership, CCPOA has been throwing millions of dollars at punitive voter initiatives. And as we learned from the Inspector General’s report and saw at the Assembly hearing, CDCR has not taken disciplinary steps against correctional officers who did not wear PPE when engaging with colleagues and with incarcerated folks. This could be the product of a members in thrall to a leadership that has been completely politically captured, Trumper-like COVID denialism among the rank and file, or both. But it needs to be firmly understood that COs who do not wear PPE and/or do not consent to getting vaccinated have no business working at CDCR facilities.
The problems with buy-in from these two populations need to be addressed immediately if there’s any hope of success with a vaccination program. Buy-in is an essential component of public health, and even if the entire prison population is prioritized–as well it should be–the vaccines are only as effective as their distribution in the population as a whole.
I will update this post with newspaper/media outlet articles about the challenges and urgency of vaccination programs in prison throughout the next few days.
Bay Area newspapers are reporting a first-of-its kind unemployment fraud, in which unemployment claims were filed, and paid, on behalf of prisoners. The latest in the series is this article from the Sac Bee, which purports to explain “How inmates pulled off giant California unemployment scam.” But even having read it, I’m unclear on what exactly happened, and especially on what they mean by “a spider web.” Here’s what we know:
Court records show a handful of inmates contacted friends and relatives on the outside, supplied them with Social Security numbers and other information, and persuaded them to file for pandemic relief on behalf of 30 different inmates. The outsiders had the unemployment payments — in the form of Bank of America debit cards issued by EDD — mailed to them.
“The cards came pre-loaded with upwards of $20,000,” said Sean Riordan, deputy district attorney in San Mateo.
Riordan said the outside accomplices then went to ATM machines and withdrew their pre-arranged cut — usually $3,000 or $4,000 — and arranged for friends or family to deliver the cards to the inmates at the jail. In one case, an outsider was found to have used an ATM in Las Vegas to collect his cut.
“It was thousands of dollars,” Riordan said.
Accomplices arranged for the remaining funds to be delivered to the inmates’ jail accounts, which could be used to buy extra toiletries or other items.
That people commit fraud, behind bars and on the outside, is not difficult to understand, and I’m sure the COVID-related deprivations and difficulties produced the kind of conditions that act as a Petri dish for these kinds of schemes. What I don’t understand is this: to what extent were the people whose names were used in this fraud (the New York Times story names Scott Peterson, convicted murderer of his wife Laci Peterson) part of the fraud? When the article say that people’s “names were used,” was it with or without their consent?
Moreover, how does all of this map onto the bigger picture of COVID relief structures? We already know that CARES Act relief is available for prisoners, because it took a lawsuit to make it happen. I also know from family members of incarcerated people that several facilities are interfering with their population’s ability to complete the claim forms. In one case I heard of, when the family member called the San Joaquin County Jail, they were told the jail would not accept any check if the IRS mails it inside, and that “they [jail staff] don’t care what law was passed.” If this is a widespread problem, as the lawsuit suggests, unemployment fraud scams appear a lot less surprising. What I want to know, though, is whether there’s some connection between the two phenomena, and whether the financial scales of the CARES Act sabotage and the unemployment fraud are on par.
If you, or a family member, are having difficulties with prisons or jails undermining your CARES Act stimulus claim, email me and tell me your story, or post it in the comments.
In essence, the argument is this: The importance of this case does not lie in some complicated, novel legal question that requires judicial review (such as in the case of contradictory decisions from lower courts): it lies in the fact that it provided a much-needed, urgent remedy for a horrific unfolding situation. The Court of Appeal’s decision was not extreme; rather, it was a measured, mild order, which leaves CDCR vast freedom to achieve population reductions at San Quentin in whatever way they see fit. The AG’s request to review the case does not offer any legal grounds to do so: they continue to argue that they did their best (without providing any expert opinion/authority supporting this claim) and that they are not bound by the findings of the AMEND team (without providing any alternative findings.)
If anything, this assertion is rather generous on the part of Von Staich’s legal team: we now know from two Inspector General reports (1, 2) that even the “commendable” measures that CDCR claimed to have taken (and was given credit for taking in the Court of Appeal decision) were not, in fact, taken in a satisfactory way.
Most importantly, the response highlights what is important about proceeding with the Court of Appeal’s remedy: the upcoming winter, which threatens a serious pandemic wave that could decimate what’s left of San Quentin unless CDCR comply with the order. More on this below.
Von Staich’s team argues that staying the proceedings in cases of people who are facing illness and death from a second wave is “precisely the wrong response at this time of crisis.” That the AG’s office’s reaction to the order–rather than hustling to save lives–was not only to appeal in Von Staich, but to ask for a stay in all the other cases, is emblematic of their breathtakingly obtuse approach to the crisis itself. At every juncture in these cases, the government has done the wrong thing: caused the outbreaks in the first place, failed miserably at taking any remedial steps, adopted the wrong administrative response, prioritized the wrong people to be released, went for short-term measures that cause outbreaks in jails and other facilities, and–which was notable in both cases–explicitly and repeatedly said that “there is no need to act hastily.” At the oral argument in Von Staich, Justice Kline responded to this with, “yes, there is. Yes, there is. There is a need to act hastily.” The measures he ordered CDCR to adopt are mild, flexible, and give them just enough rope to continue doing the wrong things (more on that in a future post.) I very much hope that the Supreme Court agrees with these response briefs that, in the face of a winter wave of COVID-19 and dire warnings for California as a whole, acting promptly (though, to our collective tragedy, far from preemptively) is exactly what we should do.
In the off-chance that anyone reading this still does not comprehend why, going into the winter holidays, urgent population reductions should be top priority not only at San Quentin, but in all CDCR facilities, here are some sobering facts. As of today, there are huge outbreaks in seven CDCR facilities:
CAL (171 new cases) CEN (50 new cases) CTF (303 new cases) HDSP (649 new cases) PVSP (319 new cases) SATF (523 new cases + the prison’s first COVID-19 death) VSP (155 new cases)
There are also new outbreaks in ten other facilities: CCC (12 new cases) COR (32 new cases) LAC (6 new cases) SOL (12 new cases) CHCF (9 new cases) DVI (3 new cases) KVSP (16 new cases) MCSP (3 new cases) NKSP (7 new cases) PBSP (6 new cases)
CDCR now “boasts” 2436 new cases per 100,000–ten times worse than the CA rate of 345 per 100,000 that has all of us hurtling toward the purple tier. The spikes in prison infections correlate with spikes in surrounding counties. We are all (sensibly) being asked to mask up, put our holiday travel plans on hold, and cook mini-feasts for our nuclear families. All of this effort and sacrifices are worthless if we continue to incubate this virus in prison. You and yours are far more at risk from aging, infirm people sitting in one of CDCR’s COVID-19 Petri dishes than you are at risk from them in the community (people age out of crime in their late 20s, and the folks most at risk from COVID are less at risk of reoffending than people on the outside.)
CDCR’s hemming and hawing about doing the right thing is not just callous disregard for the lives of people behind bars, but also for your life and mine.
In anticipation of our upcoming symposium about COVID-19 and mass incarceration, here are a few sources that our attendees might like to read. It’s not an exhaustive list; rather, it focuses on some of the themes we will be covering throughout the symposium.
Three UC Hastings journals are coming together to organize an important symposium on incarceration and healthcare, focusing on the COVID-19 prison crisis. We are excited to invite you–details will follow. For now, please SAVE THE DATES!
When?
Feb. 5, 12-4pm: California Correctional Crisis, Meet COVID-19
Feb. 12, 12-4pm: Focus on reproductive justice, trans incarcerated people, and special populations
Feb. 19, 12-4pm: Focus on immigration detention and healthcare