After a spike in early June and an apparent abatement, COVID-19 is once again tearing through the California Institute for Women (CIW) in Chino. In the last 14 days, the prison tested 1,200 of its 1,413 residents (housed in a facility designed to hold 1,398 people – slightly above 100% capacity.) The testing count on the tracking tool seems to suggest testing done in batches, but we don’t know how they are managing isolation in a crowded facility–hopefully not taking a page from the book of this women’s prison in Texas.
CIW is of special interest to me, because a few days ago we learned that Leslie van Houten, who is serving her sentence there, has been yet again recommended for parole. Van Houten has been consistently recommended for parole since 2017, but governors–first Brown, now Newsom–keep reversing the recommendation for what seems to me, after having pored over 50 years’ worth of her prison record, purely political reasons. Van Houten has maintained a clean disciplinary record, participated in a variety of laudable programs, and incessantly excavated her psyche to show “insight” to the Board. She participated in the murders when she was 19 years old, manipulated and sexually exploited in a setting that, with today’s #MeToo sensibilities, might have shed a completely different light on her involvement.
I mention van Houten’s case because it is emblematic of the dilemma that Gov. Newsom faces with countless other cases. The right thing to do is to release older prisoners, who are more vulnerable to the virus; these people, who serve long sentences, are serving them for violent crimes they committed decades ago. Everything we know about life course criminology supports the prediction that they pose no risk to public safety–they themselves face a risk by remaining behind bars.
In Yesterday’s Monsters I explain how the Manson family cases came to shape California’s extreme punishment regime, and how these cases were impacted by this new regime in turn. This is the chance for a politician who has consistently ran, and prevailed, on a platform of doing the right thing in the face of baseless political pressures. There is no ambiguity about the right thing to do now. Van Houten is 70 years old, has been consistently found to pose very low risk to public safety by actuarial instruments and by everyone who has interacted with her, and there’s a pandemic going on.
Van Houten is not the only person at CIW facing these risks. Just a few days ago, advocates were overjoyed to welcome home Patricia Wright, a 69-year-old cancer patient who doctors say has mere months to live, after she served 23 years in prison. Wright’s release encouraged me, given the infuriating and heartbreaking scene just eleven years ago at Susan Atkins’ last hearing. Perhaps the pandemic is driving home, finally, the message that allowing an older person to die at home with their loved ones, or live out in peace the few years they have left, is not a weakness, nor a slight to the victims. Perhaps it is driving home the message that compassion is an essential component of our humanity. Will Gov. Newsom choose to do the right thing for van Houten and other women at CIW, from both public health and public safety perspectives, or will he succumb to unfounded public pressure, hysteria, and fear?
Local news are ablaze with Santa Clara County District Attorney Jeff Rosen’s announcement from Wednesday, according to which his office will no longer seek the death penalty. The Chron reports:
Rosen said the change in policy was inspired by trips to Montgomery, Ala., first with a faith-based group and then with his family. After visits to civil rights museums and historical sites, Rosen said, he learned not only about slavery, but also what he called “the abhorrent misuse of the death penalty” against people of color.
“In the past, I supported the death penalty when I viewed heinous murders through eyes of the victims and families of those whose lives were taken,” Rosen said. But in recent weeks, “I have tried to look at this issue through the lens of race and inequity.
“These cases use up massive public resources and cruelly drag on for years with endless appeals that give no finality to the victims’ families,” he said. “There’s the tragic but real risk of wrongful conviction. And, shamefully, our society’s most drastic and devastating law enforcement punishment has been used disproportionately against defendants of color.”
Michael Cabanatuan, “Santa Clara County DA Jeff Rosen no longer to seek death penalty,” San Francisco Chronicle, July 22, 2020
Things I learned from colleagues who study progressive prosecution and are in the know about Santa Clara County: Rosen is facing a challenge in the form of a more progressive candidate for D.A., and apparently he has been hiring the people that Chesa Boudin fired upon becoming San Francisco’s D.A. Frankly, if the outcome is real reform–ending cash bail, establishing an integrity team to investigate criminal police misconduct, and requiring deputy district attorneys and the office’s investigators, who are currently required to take police ridealongs, to also visit communities, whether the motives are pure or not does not interest me (they never can be with elected officials.)
But this decision raises some bigger questions about the prosecutors who still pursue capital trials despite the fact that we have a moratorium on the death penalty and, actually, no longer have a working death chamber at San Quentin (see image above.) Why are we still paying the enormous expense of capital trials and appeals as if we have a functional capital punishment? Perhaps because some county prosecutors are still behaving as if we have it–as late as last month, apparently, the California District Attorneys’ Association held a webinar on “changes to execution protocols, including California’s.” As members of the CDAA know full well, the “changes” in California consist of the fact that we no longer have an actual room with equipment to conduct executions, nor do we have the chemicals we squabbled for decades about, to the tune of billions of dollars in litigation.
I can see how, in some cases, district attorneys might feel the need to signal to their constituents that they consider this or that homicide case particularly heinous by publicly seeking capital punishment; however, as the L.A. Times explains here, even with someone with a shocking record of homicides like the Golden State Killer, there is no point in a death penalty that has no meaning whatsoever. Why capital punishment? So that DeAngelo can spend the rest of his years litigating our tax money away and die a natural death, like the vast majority of deaths on death row? What would be the point?
Rosen and other prosecutors are making the only practical choice under the circumstances. Even if you are a believer in capital punishment, as any New Age guru worth their salt will tell you, you have to let go of what no longer serves you.
Today’s Chronicle features a great article by Bob Egelko, which tries to parse out who is responsible for the San Quentin catastrophe. Getting into the chain of command that made the botched transfer decision might come in handy at a later date, I think, when the time comes to file the inevitable (and more than justified) lawsuit. But, as I said in the article, the time to squabble over who’s at fault has not come yet. Right now we must have all hands on deck, including Gov. Newsom, Mr. Kelso, and Mr. Diaz, making prison releases their absolute top priority.
By now, regular readers of my COVID-19 prison crisis posts know that Gov. Newsom’s plan to release a mere 8,000 people over the course of the summer will not suffice to curb infections, illnesses, and death in prison. You also know that, at least with regard to San Quentin–an antiquated facility that lacks proper ventilation–the physicians at AMEND recommended an immediate population reduction by 50%. But how is it to be done?
The #StopSanQuentinOutbreak coalition, and the Prison Advocacy Network (PAN) have useful, well-researched answers, which are encapsulated in the lovely infographic above. Here are the coalition’s demands, and here’s the PAN page offering legal resources and pathways to release. I want to spend this post getting into the particulars. Before doing so, though, I need to explain a few important things.The Prisoner Advocacy Network has a list of pathways to release.
A lot of the categories in Newsom’s current release plan make sense and show evidence of public health thinking. They are considering age, medical condition, and time left on people’s sentences. The problem with the categories is that they are unnecessarily restrictive, and I think the restrictions can be attributed to two hangups that many people, including well-meaning, educated folks, share about prison releases: the fear that releasing a lot of people is going to be hugely expensive and the hangup around the violent/nonviolent distinction. So let’s tackle these two first.
Get over the hangup of re-entry costs. You may have read that BSCC is considering offering $15 million to CDCR, and might wonder how we can possibly pay for housing, temporary or permanent, of tens of thousands of people. Of course this is going to cost money; the question is, compared to what. It may shock you to learn that, in the 2018/2019 fiscal year, the Legislative Analyst’s Office estimated that the average cost to incarcerate one person in California for a year was $81,502 – more than a $30k increase since our recession-era prison population reduction in 2010-2011. How much does it cost to help such a person for a year, when their healthcare is funded by Obamacare, rather than by CDCR? Here’s a PPIC report from 2015 detailing alternatives to incarceration. Specifically with regard to COVID-19-related reentries, here’s another great infographic detailing what the needs are going to be. The big one is housing, and there are organizations on the ground that are set up to help with that. Even with transitional housing costs, this does not add up to $80k per person per year.
Get over the hangup of making the violent/nonviolent distinction. I am still seeing lots of well-intentioned folks who read Michelle Alexander years ago tweeting about how ending the war on drugs (with or without the hashtag), or focusing on so-called “nonviolent inmates” is the key to fighting this outbreak. I can’t really fault them for this misapprehension–what I can do is repeatedly present you with facts to correct it.
Take a look at the graph below. It comes from CDCR’s population data points from 2018. You will note that the vast majority of people in California prisons are serving time for a violent offense. Drug convictions are the smallest contributors to our prison population (this is of course not true for jails or for federal prisons; I’m talking about the state prison system.) I know we all love to say “dismantle” these days, but dismantling the war on drugs will do very little to reduce state prison population.
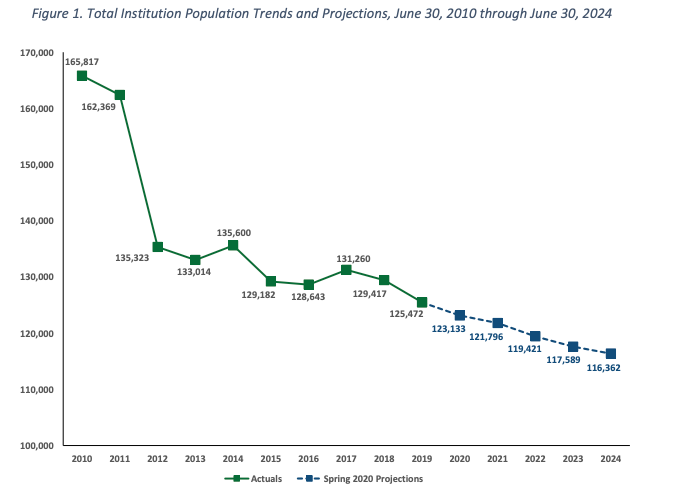
Now, take a look at CDCR’s Spring 2020 population projection. What you see in the diagram below are the reductions in population since 2010, and some projections for the years to come. The two big reductions were in 2011, following the Realignment, and, to a smaller extent, in 2015, following Prop. 47. Both of those propositions diverted drug offenders to the community corrections systems–jails and probation. If you care about the injustices of the war on drugs, your heart is in the right place, but this is simply not the most dire problem we are facing in the context of prison population reduction.
It is easier to talk about drugs and nonviolent offenders, because these are typically categories of people that evoke more sympathy from the press. My colleague Susan Turner at UCI has shown that risk assessment tools, when used properly and carefully, yield dependable predictive results, and these are not correlated with the crime of commitment. Because we were so married to the idea that only nonviolent folks need help and public support, our three major population reduction efforts–Realignment, Prop 47, and Prop 57–missed the mark on getting more reductions for little to no “price” of increased criminal activity. Whenever you see a headline lambasting the Governor or the Board of Parole Hearings for releasing a “murderer,” immediately ask yourself the two relevant questions: (1) How old is this person now, and (2) how long ago did they commit the crime? The answers should lead you to the robust insights of life course criminology: People age out of violent crime by their mid- to late-twenties, and at 50 they pose a negligible risk to public safety. Moreover, what a person was convicted of doesn’t tell you a full story of what their undetected criminal activity was like before they were incarcerated. Take a look at the homicide solving rates in California, as reported by the Orange County Register in 2017–a bit over 50%–and ask yourself whether the crime of conviction is telling you a story with any statistical meaning.
In short, my friend, take a breath, let go of your attachment to the violent/nonviolent distinction, and let’s find some real solutions. The #StopSanQuentin coalition has a more in-depth breakdown to offer. Generally speaking, the legal mechanisms to achieve this reduction were identified by UnCommon Law in their letter to the Governor–primarily, early releases, commutations, and parole. Section 8 of Article V of the CA Constitution vests the power to grant a “reprieve, pardon, or commutation” in the Governor. The Penal Code elaborates and explains the process. Section 8658 of the California Government Code provides an emergency release valve: “In any case in which an emergency endangering the lives of inmates of a state, county, or city penal or correctional institution has occurred or is imminent, the person in charge of the institution may remove the inmates from the institution. He shall, if possible, remove them to a safe and convenient place and there confine them as long as may be necessary to avoid the danger, or, if that is not possible, may release them. the Governor has the authority to grant mass clemencies in an emergency.”
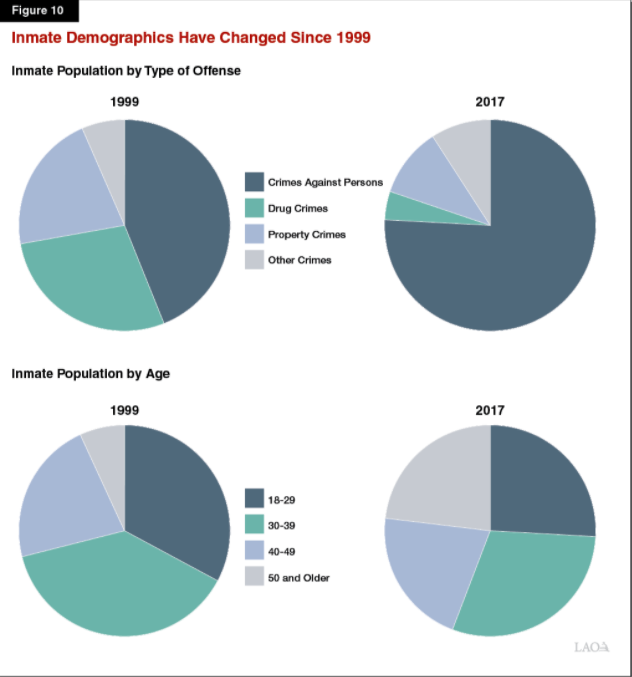
To begin, there are some bulk populations which, if targeted for release, can deliver the kind of numbers we need to stop the epidemic. These three populations largely overlap, which might make it easier to tailor the remedies to capture the right people. About half of the CDCR population are people designated “low risk” by CDCR’s own admission. CDCR uses risk classification primarily for housing purposes, and their methodology–as well as their practice of overriding their own classification–have been found by LAO to be in dire need of overhaul. LAO and other researchers believe that CDCR’s use of the “low risk” category is too restrictive, and their exceptions to their own classification come from hangups around issues of crime of commitment. This chart from the LAO report tells a useful story: Most of our prison population is doing time for violent crime, and a quarter of it is 50 and older; given the length of sentences for violent crimes, and the fact that a quarter of CA prisoners is serving decades on one of the “extreme punishment trifecta” of sentences (death, LWOP, or life with parole), it’s not difficult to figure out where the older, lower risk people fit in.
Between a quarter to a third of the prison population, depends on how you count: People who have already served a long sentence. This is the time to question the marginal utility of serving a few more years after being in prison for decades. According to the Public Policy Institute of California, About 33,000 inmates are “second strikers,” about 9,000 of whom are released annually after serving about 3.5 years. Another 7,000 are “third strikers,” fewer than 100 of whom are released annually after serving about 17 years. Approximately 33,000 inmates are serving sentences of life or life without parole. Fewer than 1,000 of these inmates are released every year, typically after spending two or more decades behind bars.
23%: People Over 50. Not only does this population intersect with lower criminal risk and higher medical risk, it also correlated with cost. According to the Public Policy Institute of California and Pew center data they cite, in fiscal year 2015 the state spent $19,796 per inmate on health care–more than thrice the national average.
To this, we can add a few smaller populations, numbering a few thousand each. Let’s start with people on death row and people on life without parole, who have been exempted from pretty much any release valve possible. The Governor has the authority to commute both of those sentences to life with parole today, and this is probably the right course of action anyway, pandemic or no pandemic. We have a moratorium on the death penalty, which means no one is getting executed but we are still paying for expensive capital punishment litigation. Cut out the middle man and shift all these folks to life with parole. I talk about how these three sentences are indistinguishable anyway in Yesterday’s Monsters, chapter 2.
There are also, apparently, a few hundred people still incarcerated who have been recommended for parole and approved by the Governor–coalition members have identified a few dozen in San Quentin alone. If these people have been given the green light to be released, why are they still behind bars? As for people who have been recommended for release and still awaiting the Governor’s authorization, now’s the time to expedite that.
Finally, lifting the offense limitations on people from outbreak epicenters, people with medical conditions, and the like, should expand those numbers considerably, given the significant overlap between crime of commitment, length of sentence, age, and health condition.
My point is that all of this is eminently doable, and there would hardly be any downsides. If we can just let go of the tendency to view only one side of the cost equation, and of our hangup about the nonviolent/violent distinction, we can scale up the proposed release plan to the point that it will be effective. Let me end with this thought: Gov. Newsom announced that the goal is to reduce San Quentin population to close to 100% of design capacity. In a sane world, prisons that are at 100% occupancy are not a goal. They are a starting point.
August 14 Update: Jason Fagone has a gorgeous piece in today’s Chron explaining how we could achieve a 50% reduction today, with negligible impact on public safety.
Today, Chad Goerzen and I looked at the new numbers from the CDCR tool and laid them over the county numbers from the L.A. Times. A few patterns emerge. First, a lot of testing is being done at San Quentin, but the vast majority of tests are coming back negative. How much we can trust this given the lag between testing date and result date is an important question, but it is at least a little bit encouraging. Second, two places in particular, which had seen peaks and valleys in infections–Avenal and CIM–are seeing infections.
For today, though, I want to point out something striking: Out of the top 15 counties in terms of infection numbers, 12 also have prisons that have seen new infections in the last 14 days. Look at the graph on the top. The picture is incomplete (we need data on detention centers and jails) but it is striking. Without contact tracing it is impossible to tell a causal story, but this correlation should be enough to easily counter the assumption that prisons are somehow separate from the community, or worse, that there’s some trade off between saving lives behind bars and on the outside. The virus doesn’t read the CA Penal Code, nor does it know where the prison gates are. Nor is there an allotted number of infections and deaths and it’s merely a question of who’s more “deserving.” If people behind prison are healthy and taken care of, people in the community are healthy and taken care of, and vice versa.
In J.R.R. Tolkien’s Lord of the Rings, the Balrog is an ancient monster, a relic from times past, who lurks beneath the surface. When the Fellowship of the Ring crosses the Bridge of Khazad-dûm, they provoke the Balrog, who angrily attacks them. Gandalf, the wizard, successfully fights the monster, but at the very last minute, as the Balrog plunges to its death, it flings its whip one last time, capturing Gandalf and dragging him along into the abyss.
The U.S. death penalty in the 21st century is like the Balrog—an ancient monster, a relic from times past, still grasping and lashing its whip even as it approaches its demise. The score, state-by-state, is even: 25 states have retained it, 22 states have abolished it, and three (including California, home to the largest death row in the country) have instated moratoria upon its use. Even in retentionist states, the rate of executions has slowed down to almost a grinding halt, and initiatives to abolish the death penalty frequently appear on the ballot. Paradoxically, as Daniel LaChance explains in his book Executing Freedom, it retains the support of the majority of people even as it loses practical ground. Much like people on death row, most of whom die natural deaths after decades of incarceration and litigation, the death penalty itself is dying a slow, natural death. This is a confluence of several factors: recession-era politics that drew attention to the immense, disproportionate expenditure on capital punishment; the rising prominence of the innocence movement, which shone a light on the widespread problem of wrongful convictions; and the Obama-era attention to racial disparities in criminal justice, among others.
Tolkien is a master storyteller, and he sets up the moment when the Balrog’s whip ensnares Gandalf as poignantly tragic—a sudden, unnecessary reminder that, even at its demise, the archaic still has bite. This is how last week felt. Taken together, the decision in Barr v. Lee and the three executions that followed were a persuasive catalogue of the evils of the death penalty, straight out of the abolitionist playbook.
First was the decision itself, which followed the expected 5-4 pattern. In the spirit and tradition of death penalty litigation in the last few decades, it revolved around what Justice Harry Blackmun referred to in the early 1990s as “tinkering with the machinery of death.” Blackmun could afford a direct, stop-beating-around-the-bush approach to the tiresome and technical minutiae of postconviction litigation, but capital defense lawyers cannot; arguments about human rights and racial disparities have long been futile, for various procedural reasons, and the limits of the sayable on appeal and on habeas revolve around chemicals and number of injections. Justice Breyer’s dissent echoed Blackmun’s distaste with what death penalty litigation has become, remarking, “[t]his case illustrates at least some of the problems the death penalty raises in light of the Constitution’s prohibition against ‘cruel and unusual punishmen[t]’”. Justice Sotomayor, in turn, remarked on the absurdity of doing justice to fundamental questions via “accelerated decisionmaking.”
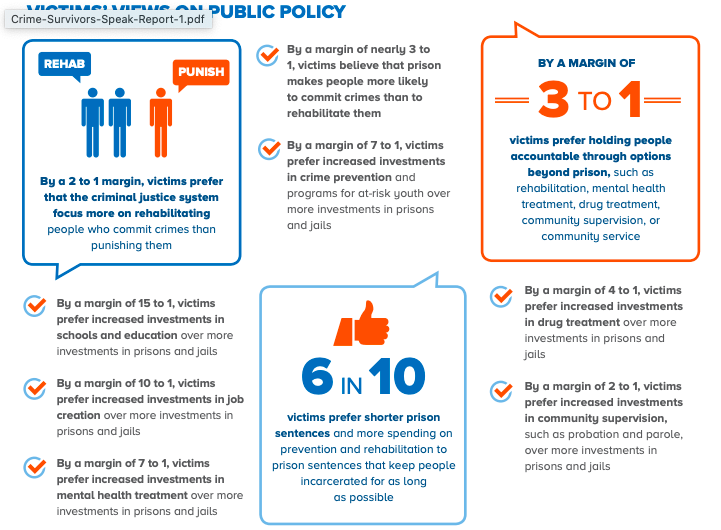
Then came the three executions, the first sneaking up on the American public while we were sleeping in our beds. Daniel Lewis Lee was put to death against the express, vocal, and repeated wishes of his victim’s families to spare him the death penalty. The judicial and executive branches’ trampling of the victim’s requests followed the usual capital punishment theater in which, as Sarah Beth Kaufman explains in her new book American Roulette, prosecutors, governors, and death penalty advocates use victims as a prop, assuming that punitiveness is faithful to their wishes. As I documented in my book Yesterday’s Monsters, in California (as in other states) the voice of victims has been captured by a small group of white, middle-class victims of stranger homicides which, albeit sincere about their own punitive sentiments, do not represent the demographics or wishes of most survivors of violent crime. The first-ever national survey of crime survivors paints a more realistic picture. Twice as many victims prefer that the criminal justice system focus more on rehabilitation than on punishment; victims overwhelmingly prefer investments in education and in job creation to investments in prisons and jails, by margins of 15 to 1 and 10 to 1 respectively; by a margin of 7 to 1, victims prefer increased investments in crime prevention and programs for at-risk youth over more investment in prisons and jails; 6 in 10 victims prefer shorter prison sentences and more spending on prevention and rehabilitation than lengthy prison sentences. The assumption that the only good victim is a punitive victim does not have a factual leg to stand on.
The execution that followed was of 68-year-old Wesley Purkey, who was described by his lawyer, Rebecca Woodman, as a “severely brain-damaged and mentally ill man who suffers from Alzheimer’s disease” and does not understand “why the government plans to execute him.” The debate over Purkey’s mental illness was emblematic of the decades and billions of dollars spent poring over the fitness of elderly, decades-long death row residents, for execution. Reading of Purkey’s execution reminded me of how COVID-19, which is ravaging San Quentin’s death row as I write this, is making a mockery of our state’s well-intended moratorium. More people on death row have died of the virus during this moratorium than have been executed by the state in the entire century, which in itself should raise serious qualms about the ethical validity of the debate whether this or that individual is healthy enough to be killed by their government.
Finally came Dustin Honken’s execution, which offered a grim reminder of the gap between the inexplicable federal enthusiasm for executions and the waning interest of states in the penalty. Honken is the first person from Iowa to be executed since 1963; Iowa abolished the death penalty in 1965. Honken’s lawyer, Shawn Nolan, said, “There was no reason for the government to kill him, in haste or at all. In any case, they failed. The Dustin Honken they wanted to kill is long gone. The man they killed today was a human being, who could have spent the rest of his days helping others and further redeeming himself.”
In her dissent, Justice Sotomayor expressed concerns about the procedural framework used to greenlight these three executions, a grant of the federal government’s emergency application, which “inflicts the most irreparable of harms without the deliberation such an action warrants.” But my deeper concern is about the inexplicable zeal that animated the emergency application in the first place. As a deadly pandemic ravages cities and towns, as the American public wakes up to the fragility of human life, the federal appetite for cheapening it by pursuing human-inflicted killings in the name of dated approaches is astounding. That it is in step with the Trump administration’s embrace of old-school punitivism does not make it any less perplexing, nor any less tragic. The Balrog of the death penalty is taking its last steps, but its last whiplash, an echo of what passed as justice in the olden days, stings as viciously as ever.
The sensation of shock, like unsavory gray smoke filling my lungs, making me nauseous with incomprehension, has stayed with me, and seems to have been universal. Dan was so alive–isn’t that what is always said of the dead?–a true, energetic community builder, the architect of Prawfs Blawg, the inaugurator of CrimFest, both of which have outlived him. A loving father to his two young boys, of whom he always spoke with such affection. The nauseating smoke whispered, how? why? who? Theories spread among Dan’s friends and colleagues; blogs were ablaze, picking up the shreds of Dan’s life, looking for some conflict, strife, danger, something that would explain the unexplainable. Underneath it all, unspoken save, perhaps, in the offices of my friends’ therapists, was the uncomfortable but true realization, this doesn’t just happen to someone I know. People living comfortable lives of safety and social advantage, lives that do not grow in the shadow of street violence or require it, were deeply unsettled. If we could only find out why, we felt, perhaps, this senseless thing will make sense; something in Dan’s life, in his relationships and entanglements, would make sense of this out-of-place death.
The mystery of Dan’s murder lingered on, picking up steam occasionally on blogs, for two years. Whenever I met other friends and colleagues of Dan’s, we shook our heads. “We just want to know what happened,” we said. The aching gap Dan left in the professional and social fabric of our trade was lovingly mended by friends who took the mantle of organizing. Then, two years later, we found out. It was sordid, disturbing, the stuff of low-grade cold-crime television shows in which a deep-voiced anchor dramatizes the events. They were Luis Rivera, 33, and Sigfredo García, 34, murderers for hire, and the only plausible connection between them and Dan was the mother of García’s children, Katherine Magbanua, who was dating a rich Florida dentist, Charlie Adelson.
Adelson was Dan’s brother in law. Dan and his ex-wife, Wendi Adelson, had divorced in 2013, and were amidst an ugly custody battle; Dan had won an order prohibiting Wendi from moving to Miami with the children, and filed a motion that would have prohibited Donna, Wendi’s mother, from being alone and unsupervised with the children due to alleged disparaging remarks about Dan. The investigators alleged Magbanua made the connection between the Adelson family and Garcia , that she received a large amount of money from the Adelsons following Dan’s murder, and that Magbanua was the first call Garcia dialed after Markel was murdered.
All this added up to arrest warrants against García, Magbanua, and Rivera, but not against the Adelsons. Despite repeated efforts to trip them, they have eluded law enforcement efforts at gathering more evidence against them. Rivera turned state witness, García was convicted, and Magbanua, who remained steadfastly silent even in the face of a threat with Florida’s death penalty, won a mistrial (ten jurors voted to convict, two to acquit.) Magbanua is to be retried for the murder. Much as I find it loathsome and distasteful to lionize and sanctify the three apprehended parties to a murder-for-hire because they are “poor people of color,” I can understand and empathize with the sentiments of injustice: the rich and powerful have managed to escape all consequences of their likely actions. Given what we know, what plausible explanation could there be for all this except the Adelsons’ desire to get Dan out of the way? Not one member of the Adelson clan evokes even a shred of sympathy: In a particularly cruel move, Wendi Adelson immediately proceeded to remove Dan’s last name from those of the children and denied them contact with their paternal grandparents. And yet, the police claims not to have cobbled enough probable cause for an arrest.
Thing is, what I think happened and what the law, which requires stringent beyond-reasonable-doubt proof, asserts happened, are two different things. The law does not operate in a vacuum, and people of means have many ways to insulate themselves from incriminating behavior and paper trails. I know many of my friends and colleagues who grieve for Dan hope for justice in the form of criminal consequences for the Adelsons. Much as I fail to comprehend the moral makeup of the Adelsons, I’ve always been pretty clear on the fact that I would not feel even a little bit better about this tragedy if I heard that the police arrested Donna, Charlie, or Wendi. Moreover, I didn’t feel relieved or vindicated when the police waved the threat of capital punishment over Katherine Magbanua’s head. Not only did it not work, in Magbanua’s case, and not only does this use of the death penalty as a bargaining tool create ugly disparities between sentences in abolitionist and retentive states, but I found the whole entanglement with the worst aspects of Florida’s criminal justice system tasteless given Dan’s own scholarly stance against the death penalty. My conversations with many of Dan’s friends and colleagues revealed that they, too, felt like knowing what had happened and making their mind about the culprits was sufficient. What horrors, albeit deserved, could the criminal justice system possibly visit upon the Adelsons that would make us feel better about the grievous loss of our friend?
I’m not particularly surprised that so many people’s grief over Dan’s death didn’t manifest as a desire to see his killers–all of them, including the ones too dainty to pull the trigger–harshly punished. I see the same from families and friends of homicide victims all the time. The first-ever national survey of crime survivors show that victims are far less punitive than Twitter would have you believe.
Not everyone is nonpunitive, of course. The Tate family, whom I discuss at length in my book Yesterday’s Monsters, were instrumental in shaping public perception of what victims want, as was Mark Klaas. I don’t think any of these people has been manipulative or insincere or has not suffered unimaginable pain; I do think, however, that their voices are mistakenly assumed to represent what most victims want, which is not the real picture. Nor is this an illness particular to the conservative right; the fault lies just as much with the folks who wrote fashionable pieces about how Jean Brandt’s act of faith and forgiveness toward Amber Guyger was “problematic” in that it “allowed whites to benefit from black forgiveness”, because some people on the left are apparently so enlightened that they can educate people on how to properly grieve their relatives. I saw the same dynamic in some of the astonishing reactions on Christian Cooper’s sane and measured response to the police investigation of Amy Cooper’s false complaint about him to the police, those accusing him of “performing a disservice” to African Americans nationwide, because apparently (1) everything has to be a performance and (2) the only true path to social justice is through arrests, charges, and convictions.
That this–a reaffirmation of our government’s commitment to a punishment that is, itself, dying a slow death (like many of death row inmates themselves)–is our takeaway from this pandemic, is mind boggling, but I see the same mentality among those wondering why we worry about people on California’s own death row catching COVID-19. Being on death row is hardly a natural consequence of one’s actions, as so many of my colleagues have explained over the years, and so the shrugging of shoulders, accompanied by a more or less crude version of “you do the crime, you do the time” or “we have to make priorities” astounds and perplexes me. As we inch toward November, the urgency of a vote that affirms everyone’s value in the dance of life becomes clearer and clearer. And then, we begin the hard work of reshaping the arc of progress, which has taken a very, very wrong turn.
Lately I’ve been thinking about environmental ethics quite a bit. I came to it through noticing patterns and values in vegan and animal rights groups, and partnering with my brilliant colleague and precious friend David Takacs to put together and teach our environmental criminology seminar has greatly deepened my interests. Early on in our work together, David and I had fascinating debates about animal ethics, in which he expressed an ecocentric worldview, whereas I took mostly a biocentric perspective. I found the logics and contradictions of my own position interesting, particularly in our debate about trophy hunting regulation, which I recounted here. Long story short, I found myself in the complicated, but ethically juicy, place of trying to reconcile my sense that each individual lion’s life is sacred and nothing short of a complete ban on hunting would reflect the purity of this fact with my understanding that the path toward protecting lions as a species and the indigenous communities that protect them might be regulation and the sale of expensive licenses. I still can’t get over the stumbling block that the lions’ lives are not ours to sell. We have created rules and economies that are alien to the way the world runs, and alien to the way in which we used to live in nature.
I’ve spent the last few months working through Joanna Macy‘s writings and attending two wonderful webinars in The Work that Reconnects. I’ve also been spending a lot of time in nature, experiencing plants, animals, and other natural kingdoms in a reverential and playful context that my pre-COVID life did not have space for. We have grown vegetables and herbs in the garden for years, but now, for the first time, I’m immersing myself in mycology and growing mushrooms (so far from kits, but it’s so interesting nonetheless.) Here’s a great documentary about the marvel of the fungal kingdom:
https://youtu.be/ZGEdHxiWo_Y
The theme that emerges from this work, which is enriching my mindfulness meditation teacher training, is interconnectedness-both as a scientific concept and as an immediate, natural, somatic understanding of relationships, cause and effect, cooperation and responsibility.
It was this sense of somatic interconnectedness that brought me to the animal rights world in the first place. I had been vegetarian for many years, interrupted by a couple of years of eating meat because I believed my endurance swimming practice required it, and then went to see Judy Irving’s marvelous documentary Pelican Dreams. The film’s starting point is a brown pelican, found starved and disoriented on the Golden Gate Bridge; Irving follows Gigi the pelican to a pelican sanctuary, and learns more about their lives on between Catalina Island and the Bay Area. Here’s the trailer:
Along the way, Irving learns that many pelicans sicken and suffocate from large surplus fish parts that commercial fisheries through back in the water. It was then that I realized that the evils of commercial consumption of animal products, and the cruelties of factory farming, were linked to evils to wildlife and the biosphere in ways that I no longer wanted to be part of. In the six years since watching the film, my family (with the exception of the cats, who, as obligate carnivores, did not choose to live with us and do not do well on vegan cat kibble) has shifted to a completely vegan diet. We cook and bake better every day and are very proud of our home cuisine, into which we bring our heritages as well as dishes from around the world, which we pick up from friends and books. My academic work on animal rights, which includes my book in progress on open rescue activism, comes from my deep personal interest in animal ethics.
A lot of the discourse in the animal rights world revolves around anthropomorphizing factory farmed animals, in much the same way that the rest of the world anthropomorphizes pets. I’m not sure that imposing our sensibilities in that way is 100% accurate, but within the limitations of human perception and language, I understand it as valuable shorthand to speak of animal rights. Many friends are shaken (in a good way) when I tell them that chickens can do math and that pigs are amazing problem solvers. But as much affection and love as I have for our nonhuman friends, my deep commitment to veganism and animal rights comes from my gratitude for the natural world as a whole, and from my deep sadness that we have grossly overstepped our place in the interconnected web of life. Animals have to feed on each other; as Peter Godfrey-Smith explains in Other Minds, interacting with each other as predators and prey was an important shift in the evolution of consciousness. But this applies to the overall sense of balance in our ecosphere, in which animals hunt and kill what they can and need to eat and no more. Our bloated, cruel apparatus of animal farming is so removed from that reality that I recoil whenever someone tries to tell me that ordering a plate of bacon or a steak is “natural.” There is nothing natural about how we do this, nothing sustainable; to refer to our horrific food supply system as part of the “food chain” is beyond offensive; and because it is so deeply out of step with everything I believe, the only resort I have is to opt out of it completely.
To be more versed in the scientific and spiritual aspects of natural interconnectedness, I’m doing a lot of wandering, and watching, and growing food, and also reading. Here are some of the books I’m enjoying lately:
Peter Godfrey-Smith, Other Minds: The Octopus, the Sea, and the Deep Origins of Consciousness
Robin Wall-Kimmerer, Braiding Sweetgrass: Indigenous Wisdom, Scientific Knowledge and the Teachings of Plants
Sy Montgomery, Soul of an Octopus: A Surprising Exploration into the Wonder of Consciousness
Paul Stamets, Mycelium Running: How Mushrooms Can Help Save the Planet
Peter Wohlleben, The Secret Life of Trees
Peter Wohlleben, The Inner Life of Animals
Peter Wohlleben, The Secret Wisdom of Nature
David Abram, Becoming Animal
David Abram, The Spell of the Sensuous
Chris Johnstone and Joanna Macy, Active Hope
Joanna Macy and Molly Young Brown, Coming Back to Life
John Seed and Joanna Macy, Thinking Like a Mountain: Toward a Council of All Beings
Rachel Carson, The Sense of Wonder: A Celebration of Nature for Parents and Children
As a postscript, I’ll mention that much of the passion behind my work to save lives of people behind bars from COVID-19, and much of my deep outrage about the three federal executions yesterday, come from befuddlement and grief. At a time in which we are seeing so much tragic destruction of human life, it is perplexing and distressing that not all of us awaken to the realization that all life, human and nonhuman alike, is sacred and calls for reverence and protection.
A couple of weeks ago I posted about the “known unknowns”: the situation in county jails. I don’t think that the cloud of ignorance over infections, illnesses, and deaths in hundreds of facilities (some as big as prisons) is coincidental. I’ve already mentioned the concept of agnotology–the study of culturally induced ignorance or doubt, particularly the publication of inaccurate or misleading scientific data–and I think that, when problems are prioritized, knowledge about them is also gathered and shared.
We have an opportunity to press the Board of State and Community Corrections (BSCC) for some answers, because they have just announced an emergency meeting scheduled for this Thursday, July 16 at 10:00 a.m. At the meeting they plan to decide whether to give $15 million of the total $58.6 million of federal Coronavirus Emergency Supplemental Funding (CESF) to the California Department of Corrections and Rehabilitation (CDCR) to “quickly leverage existing contracts that can provide emergency housing” for individuals being released from state prison due to COVID-19. You can find the full proposal here; the gist of it is as follows:
In May, the BSCC’s CESF application for $58.5 million was approved. In June, the BSCC launched a dedicated CESF email address to seek input on how the funds should be used, established a 30-day public comment period that concluded July 12, and staff committed to sharing those results with the Board at the September Board meeting. In the weeks following the June Board meeting, however, the Administration identified an urgent need to provide housing to individuals being released from CDCR due to COVID-19. As many as 8,000 individuals with less than a year left on their sentences could be eligible for release by the end of August. There is an immediate need for housing to help these people with successful reentry. The Administration has requested a portion of the federal grant to meet those emergency needs.
A CESF award would allow CDCR to immediately leverage existing contracts through the Specialized Treatment for Optimized Programming (STOP) to help with emergency housing needs. The STOP system operates in six regional areas statewide, with offices in LA, San Diego, Sacramento, Marin, San Bernardino and Fresno. Each provider contracts to provide step-down services ranging from residential treatment to recovery and reentry housing at the local level. The proposed funding would provide emergency housing and could cover costs associated with increasing housing capacity and providing quality assurance of housing to ensure safe housing standards are implemented.
The Board will have the opportunity to consider the public comment received to determine priorities for the remaining $41.7 million and take further action at the September meeting. Sixty-seven public comments have been received to date from community based organizations, local governments (both city and county), concerned citizens, public and private organizations, law enforcement, and the faith-based community.
This, in itself, might be a good thing–the money will be sorely needed to cushion the path of so many folks who have been incarcerated in an environment that is an anathema to rehabilitation as they make their first steps in a horrible economy. But we must also be mindful of the fact that we don’t actually know what the situation is in jails, and to what extent these funds are needed to put out local COVID fires on the county level. In any case, if you want to chime in and make your opinions known at the meeting tomorrow, here’s all the info you need to attend the emergency meeting. I’m not sure I can make it, but if I could, my priority would be to comment on the fact that BSCC must be the “responsible adult” and liaise between the counties to create a uniform, informative reporting platform for all the jails in California. We cannot solve a problem we know so little about.
Important postscript: The last few weeks have made the question of school reopening into yet another partisan screeching war lacking any nuance. While we have proof (not unambiguous, because this virus is a shapeshifter when it comes to data) that indiscriminate school reopening without social distancing measures can be dangerous, we also have proof that early education centers (daycares and preschools) that have rigorous sanitation and distancing protocols in place have not contributed to the spikes we are seeing (in fact, many of them were operating for months, for children of first responders, without seeing positive infections.) The most shrill, uncompromising voices for not opening schools come from what some might consider “my” side of the political map, and almost without exception from people who (1) don’t have kids (2) don’t teach kids and (3) don’t work in K-12 school administration. I’m noticing that these posts, invariably strewn with expletives about the selfishness of opening schools, are harvesting “likes” aplenty, because apparently wanting children to be properly educated and socialized, regardless of their class or wealth, is suddenly no longer a progressive priority, and wanting abuse, neglect, and household poverty to be detected and addressed is tantamount to being a loathsome Trumper. There are many good and knowledgeable people in school administration–some of them are good friends of mine–and they report so much uncertainty and efforts to do the right thing, precisely because they are exposed to the downsides of multiple options. There’s complicated choreography and architecture and proper messaging that needs to be done. I don’t have the answer to the difficult questions (and anyone who claims they have the perfect solution is either lying or ignorant), but I will tell you this: everything you’ve seen from me in the last three weeks—TV appearances, radio appearances, newspaper stories, dozens of posts with primary data analysis, this morning’s op-ed in the Chronicle, the open letter, the press conference speech–everything that I have done to try and save lives behind bars–has been brought to you by my son’s preschool, which has been open now for three weeks, and thank goodness for that. To their great credit, they took on an enormous amount of work and created sanitation protocols, symptom checking lines, pick-up and drop-off routines, and rigorous cohorting, so that I can write this post and you can read it. Working parents are part of the economy and part of the community. When we are full-time caregivers for our children, we are excluded from contributing to our communities in other ways. You might want to think of that and square the struggle to stop the prison outbreak with other progressive sensibilities before you exhort your local government to make decisions that lack nuance, ignore externalities (to teachers as well as students and families.) For more on why it is important to say this, read here.
Trump is not the only president to have used his commutation powers in controversial ways. As this excellent NPR piece explains, both Bushes and Clinton were criticized for misuse of their powers, as was Obama for the sheer number of commutations. What is unique about Trump’s pardons and commutations is that, with a handful of exceptions, they were given to people in furtherance of his own personal interests or to people prominently featured on Fox News. Moreover, Trump has virtually ignored the Department of Justice’s Office of the Pardon Attorney, whose function is to parse out the thousands of pardon requests it receives every year and make recommendations to the President. Usually, the President follows the Office’s recommendations, but not in this case, and as Mitch Jeserich and I discussed this morning on KPFA’s Letters and Politics, this means not only that Trump’s business partners and go-betweens are rewarded for their crimes, but also that ordinary people’s petitions are ignored and recommendations about them go unheeded. Trump’s adulation and courtship of celebrities is one contribution to his assault on the rule of law (with the notable exception of Kim Kardashian’s influence on the First Step Act). Combine all of this with Bill Barr’s jockeying of Manhattan federal prosecutors and you’ll find a continuation of the same trends.
One issue that Mitch and I discussed today was the public discourse around Roger Stone’s age and (he’s 67), and the argument that, with the pandemic ravaging prisons, he would be “put at serious medical risk in prison“. Of course age and health condition are valid considerations, but let’s keep things in context. Here’s a breakdown of the federal prison population by age. Close to 20% of them are aged 51 and older. Throw in people aged 46 and above, and you’re at almost a third of the prison population. That’s tens of thousands of people. One person, albeit famous/infamous, is a drop in the bucket, so forgive me if I’m not persuaded by the argument that this reflects sensitivity to public health.
Source: Federal Bureau of Prisons, https://www.bop.gov/about/statistics/statistics_inmate_age.jsp
Worried about older people catching COVID-19 in federal prisons? Let them go–not only the ones that are doing time for being presidential go-betweens, but those who are doing time on a Frankenstein-like construction of enhancements and multiplications on nonviolent drug offenses (this is not as much of a thing in state prisons, but it is a huge factor in federal ones).
Speaking of state prisons, the situation at San Quentin continues to be dire. Over the weekend, they’ve seen 204 new cases. Notably, those are 204 positives out of a total of 259 tests, so things are going horribly wrong there. There are also 167 new cases at CCC (reflecting a major testing push), 15 new cases at CCI (hundreds of new tests there, as well as in DVI), 8 new cases at CRC, 5 new cases at WSP, 1 new case at SOL, 1 new case at CAL, and 2 new cases at CHCF (this is particularly worrisome because this Stockton prison houses a medically vulnerable population.)
In short, gentle readers, things are not going well. Stay tuned for updates.
CDCR’s plan for releasing 8,000 explained. It will provide essential relief to some incarcerated people and their families, but it is too little, too late, too reactive, and too tailored to public pressure.